Nursing Care Plan (NCP) for Eating Disorders (Anorexia Nervosa, Bulimia Nervosa, Binge-Eating Disorder)
Included In This Lesson
Study Tools For Nursing Care Plan (NCP) for Eating Disorders (Anorexia Nervosa, Bulimia Nervosa, Binge-Eating Disorder)
Outline
Lesson Objective: Nursing Care Plan for Eating Disorders (Anorexia Nervosa, Bulimia Nervosa, Binge-Eating Disorder)
Eating disorders are complex mental health conditions that require a comprehensive and sensitive approach from healthcare professionals.
- Understanding the Spectrum of Eating Disorders:
- Develop a nuanced understanding of Anorexia Nervosa, Bulimia Nervosa, and Binge-Eating Disorder, recognizing their unique characteristics, diagnostic criteria, and potential physical and psychological consequences. Appreciate the diversity within the spectrum of eating disorders and the impact on individuals’ lives.
- Holistic Assessment and Diagnosis:
- Hone assessment skills to identify signs and symptoms associated with different eating disorders. Focus on gathering comprehensive information about dietary habits, weight history, body image perceptions, and psychological well-being. Enhance the ability to recognize warning signs and facilitate early diagnosis.
- Individualized Care Planning:
- Develop individualized care plans tailored to the specific needs and preferences of individuals with eating disorders. Emphasize a person-centered approach that addresses not only the physical aspects of the disorder but also the psychological and emotional components. Consider collaborating with mental health professionals for a holistic treatment plan.
- Nutritional Interventions and Monitoring:
- Gain proficiency in providing nutritional interventions that promote a balanced and healthy relationship with food. Understand the nutritional requirements for individuals with eating disorders and develop monitoring strategies to address nutritional deficiencies, electrolyte imbalances, and other potential complications.
- Psychosocial Support and Therapeutic Communication:
- Cultivate effective therapeutic communication skills to establish rapport and trust with individuals experiencing eating disorders. Explore strategies for providing psychosocial support, addressing body image concerns, and fostering positive self-esteem. Understand the role of family and support networks in the recovery process.
- Prevention, Education, and Collaboration:
- Emphasize preventive strategies and health education to raise awareness about the risks and consequences of eating disorders. Collaborate with interdisciplinary teams, including psychologists, dietitians, and mental health specialists, to ensure a comprehensive and coordinated approach to care.
Pathophysiology of Eating Disorders
- Anorexia Nervosa:
- Characterized by self-imposed starvation and extreme dietary restriction, leading to insufficient energy intake.
- Altered neurobiological mechanisms, including disturbances in serotonin and dopamine levels, contributing to obsessive thoughts about body weight and shape.
- Hormonal imbalances, such as low levels of gonadal hormones (estrogen, testosterone), resulting in amenorrhea and impacting bone health.
- Changes in neurotransmitters, particularly elevated cortisol levels, influencing stress response and potentially exacerbating anxiety.
- Bulimia Nervosa:
- Involves recurrent episodes of binge eating followed by compensatory behaviors like vomiting, excessive exercise, or laxative use.
- Dysregulation in the reward pathways of the brain, with an increased sensitivity to food cues and reduced ability to control impulsive behaviors.
- Electrolyte imbalances due to purging behaviors, leading to potential complications like hypokalemia and cardiac arrhythmias.
- Gastrointestinal complications, such as esophageal inflammation and tooth decay, resulting from repeated episodes of vomiting.
- Binge-Eating Disorder:
- Marked by recurrent episodes of consuming large quantities of food without compensatory behaviors.
- Dysregulation of appetite-regulating hormones, such as ghrelin and leptin, contributing to episodes of excessive eating.
- Altered neural pathways related to reward and pleasure, similar to those seen in other addictive behaviors.
- Increased risk of obesity and related metabolic conditions due to the consumption of large amounts of high-calorie foods.
- Commonalities Across Disorders:
- Disturbances in body image perception, involving a persistent dissatisfaction with one’s shape and weight.
- Genetic predisposition, with heritability playing a role in susceptibility to eating disorders.
- Psychosocial factors, such as societal pressures, trauma, or interpersonal issues, contributing to the development and maintenance of disordered eating behaviors.
- Physical Complications:
- Shared physical consequences across eating disorders, including malnutrition, electrolyte imbalances, cardiac irregularities, and gastrointestinal issues.
- Neurological changes, such as brain atrophy and cognitive impairment, resulting from inadequate nutrition and potential dehydration.
- Endocrine disruptions affecting the hypothalamic-pituitary-gonadal axis, leading to hormonal imbalances with consequences for reproductive health.
Etiology of Eating Disorders
Diagnostic Criteria:
Anorexia Nervosa
- Restriction of nutritional intake that leads to significant low body weight
- Intense fear of gaining weight or becoming fat
- Altered perception of body weight or shape
Bulimia Nervosa
- Recurrent episodes of binge-eating and BOTH:
- Eating a larger amount of food in a short period of time than normal
- Lack of control over eating
- Recurrent purging: self-induced vomiting, misuse of laxatives, diuretics, fasting or excessive exercise
- Binge-eating and purging both occur at least once a week for 3 months
- Self perception is unreasonably influenced by body shape and weight
Binge-Eating Disorder
- Recurrent episodes of binge-eating and BOTH:
- Eating a larger amount of food in a short period of time than normal
- Lack of control over eating
- Binge-eating episodes are associated with 3 or more of the following:
- Eating quickly, until uncomfortably full, or alone due to embarrassment
- Eating large amounts of food when not physically hungry
- Feeling disgusted with oneself or guilty afterward
- Marked distress regarding binge-eating
- Binge-eating occurs at least once/wk for 3 months
- Binge-eating is not associated with purging
Desired Outcomes for Eating Disorders
- Normalization of Eating Patterns:
- Achieve regular and balanced eating habits, including the incorporation of all essential food groups, to support overall nutritional health.
- Healthy Weight Restoration:
- Attain and maintain a weight that is appropriate for age, height, and body composition, promoting physical well-being and preventing complications associated with malnutrition.
- Improvement in Psychological Well-Being:
- Enhance self-esteem, body image, and overall mental health by addressing distorted thought patterns, fostering self-acceptance, and promoting positive coping mechanisms.
- Development of Coping Skills:
- Acquire adaptive coping strategies to manage stress, emotions, and life challenges without resorting to disordered eating behaviors, promoting long-term emotional resilience.
- Enhanced Interpersonal Relationships:
- Improve communication and relationships with family, friends, and support networks to create a positive environment that reinforces recovery and sustains long-term well-being.
Eating Disorders (Anorexia Nervosa, Bulimia Nervosa, Binge-Eating Disorder) Nursing Care Plan
Subjective Data:
- Obsession with calories or fat content of foods
- Depression
- Fear of gaining weight
- Denial of low body weight
- Constipation
- Feeling cold most of the time
- Feeling tired
- Muscle weakness
- Chronic sore throat
- Abdominal pain
- Eating alone or in secret
- Frequent dieting
*Note – the presence of these symptoms individually do not indicate an eating disorder, assess the full clinical picture.
Objective Data:
- Restricted eating
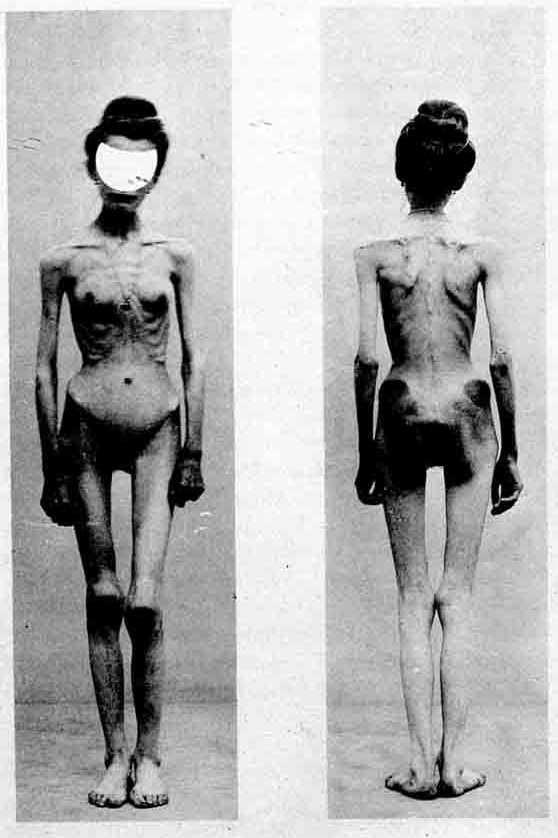
- Emaciation
- Low blood pressure
- Infertility
- Lethargy
- Brittle hair and nails
- Dry, yellowing skin
- Muscle wasting
- Thinning bones
- Eating very fast
- Growth of hair all over the body (lanugo)
Nursing Assessment for Eating Disorders
- Nutritional Status Assessment:
- Conduct a thorough nutritional assessment, including dietary habits, food preferences, and any restrictive behaviors. Monitor weight changes, dietary patterns, and identify nutritional deficiencies.
- Physical Health Evaluation:
- Assess vital signs, hydration status, and signs of malnutrition. Monitor electrolyte levels, cardiac function, and complications associated with eating disorders, such as amenorrhea or gastrointestinal issues.
- Psychosocial Assessment:
- Evaluate the individual’s mental health, including mood, anxiety levels, and presence of co-occurring psychiatric conditions. Explore body image perceptions, self-esteem, and stressors contributing to disordered eating.
- Behavioral Observation:
- Observe eating behaviors, including rituals, avoidance, or binge-eating episodes. Note any evidence of purging behaviors, such as self-induced vomiting or excessive exercise.
- Risk Assessment:
- Assess the risk of self-harm, suicidal ideation, or other safety concerns. Identify the level of social support and potential stressors contributing to the maintenance of the eating disorder.
- Cognitive Functioning:
- Evaluate cognitive abilities, concentration, and decision-making. Identify cognitive distortions related to body image, weight, and food that may contribute to the eating disorder.
- Family Dynamics:
- Explore family dynamics and relationships, as family support and involvement can significantly impact recovery. Identify any family patterns that may contribute to the development or maintenance of the eating disorder.
- Cultural and Societal Influences:
- Consider cultural and societal factors influencing body image and eating behaviors. Explore the impact of societal standards on the individual’s self-perception and attitudes toward weight and appearance.
Implementation of Eating Disorders
- Collaborative Treatment Planning:
- Work collaboratively with the interdisciplinary team, including physicians, dietitians, psychologists, and other healthcare professionals, to develop a comprehensive treatment plan tailored to the individual’s needs.
- Nutritional Counseling and Education:
- Provide ongoing nutritional counseling and education, focusing on promoting a balanced and healthy relationship with food. Collaborate with a registered dietitian to develop meal plans that address nutritional deficiencies and support weight restoration or maintenance.
- Psychotherapy and Counseling:
- Implement evidence-based psychotherapeutic interventions, such as cognitive-behavioral therapy (CBT), dialectical behavior therapy (DBT), or family-based therapy (FBT), to address underlying psychological factors contributing to the eating disorder.
- Monitoring and Support:
- Establish a regular monitoring schedule for vital signs, weight, and laboratory values. Offer continuous support and encouragement to the individual during meal times, addressing any challenges or anxiety associated with food intake.
- Promotion of Self-Care and Coping Strategies:
- Facilitate the development of healthy coping mechanisms and self-care strategies to manage stress, anxiety, and emotional triggers. Encourage the exploration of alternative ways to express emotions and build resilience.
Nursing Interventions and Rationales
- Perform complete nursing assessment noting skin, muscle tone and neurological status; include weight (BMI) and vital sign assessment
Get a baseline for effectiveness of interventions. Note any deficits or other issues that may need to be prioritized.
Determine severity of condition.
- Assess nutritional status and set a weight goal
Determine if client is under or over weight and nutritional needs
- Assess client for depression and suicide potential
Clients with eating disorders often have accompanying depression with suicidal thoughts. Monitor for safety.
- Supervise client during meals and for at least one hour after eating (in inclient treatment)
Determine client’s eating habits and prevent purging after meals.
- Encourage liquid intake over solid foods
Eliminates the need to choose foods, provides hydration and is more easily digested.
- Provide small meals and snacks appropriately
Prevents bloating and discomfort in clients following starvation and encourages eating more appropriate portions.
- Monitor for signs of food hoarding or disposing of food.
Clients may try to hoard food for secretive eating or dispose of food to avoid calories.
- Monitor exercise program and set limits and goals accordingly
Moderate exercise helps maintain muscle strength and tone, but excessive exercise burns too many calories and contributes to clients’ disorder.
Alternatively, lack of exercise can lead to depression, muscle wasting and increased weight and a negative self image.
- Administer TPN supplemental nutrition as appropriate
In cases of severe malnourishment and life-threatening situations, TPN may be used to maintain gastric function and provide nourishment.
- Monitor fluid balance and administer oral and IV fluids as appropriate
Failure to eat or drink and repeated purging through vomiting or excessive use of laxatives can cause a fluid imbalance and lead to dehydration. Prevent electrolyte imbalances and cardiac involvement by maintaining adequate hydration.
- Record routine weights per facility protocol
Monitor progress of interventions and incorporate routine accountability checks for clients.
- Monitor skin for wounds, dryness, excoriation or deep tissue injuries
Lack of hydration and proper nutrition lead to decreased perfusion and poor circulation. Dryness and itching is common. Wounds may develop over bony prominences.
- Administer medications appropriately
- SSRI antidepressants
- Anti-anxiety medications
- Psychostimulants
Medications may help relieve the underlying conditions that increase symptoms by improving mood and thinking.
Psychostimulants have proven helpful in studies to help treat binge-eating disorder and maintain weight.
Some medications may be given to curb appetite so that cognitive behavior therapy may be more effective.
- Provide education for clients and family members regarding disease, treatment and support resources
Help client and family members make informed decisions and reduce stress and anxiety about treatments. Provide opportunity for continued support and therapy for optimal recovery.
Evaluation for Eating Disorders
- Physical Health Assessment:
- Regularly assess and monitor the individual’s physical health, including weight, vital signs, and laboratory values, to determine progress in achieving nutritional stability and overall well-being.
- Psychological and Behavioral Evaluation:
- Evaluate changes in psychological and behavioral patterns, such as attitudes towards food, body image, and engagement in disordered eating behaviors. Utilize standardized assessment tools to measure improvements in mental health.
- Collaborative Team Feedback:
- Seek feedback from the interdisciplinary team, including input from physicians, psychologists, dietitians, and other professionals involved in the care. Evaluate the effectiveness of the treatment plan through regular team meetings and discussions.
- Client and Family Input:
- Encourage open communication with the individual receiving care and their family. Obtain feedback on their perception of progress, challenges faced, and areas of improvement. Consider their insights in the overall evaluation process.
- Long-Term Outcome Monitoring:
- Establish long-term outcome measures to assess sustained recovery and relapse prevention. Monitor the individual’s ability to maintain a healthy relationship with food, achieve and maintain a stable weight, and engage in positive coping strategies.
References
- https://www.opalfoodandbody.com/wp-content/uploads/2016/01/summary-of-dsm-5.pdf
- https://www.nimh.nih.gov/health/topics/eating-disorders/index.shtml
- https://npwomenshealthcare.com/continuing-education-practical-strategies-for-the-diagnosis-and-management-of-binge-eating-disorder/
Transcript
Hey guys, in this care plan, we will cover eating disorders, including anorexia nervosa, bulimia nervosa and binge eating disorder. So, in this eating disorders care plan, we will cover the desired outcome, the subjective and objective data along with the nursing interventions and rationale for each.
Let’s explore the different eating disorders. Anorexia nervosa consists of restricting the food that they’re eating, so they’re not going to be eating very much at all. This is going to lead to significantly low body weight. Bulimia nervosa will also lead to low body weight, but the difference is they’re going to eat, but then they’re going to purge. They’re going to vomit it all out afterwards. Eating disorders such as binge eating are a little bit different. So, this is where the patient is just going to eat a lot and they’re not purging afterwards. They’re eating a lot. They might be a little larger in size, right? They’re going to gain weight and then they’re going to feel really guilty afterwards. So, eating disorders often coexist with other mood disorders or personality disorders, such as substance abuse, and they involve an altered perception of their weight or uncontrolled eating. The patient’s going to verbalize an understanding of their nutritional needs after we’re done with them. That’s our “what” that we’re hoping for right? We want them to improve their weight toward the normal range, whether it’s larger or smaller, and they need to establish a realistic body image. We need them to realize that they’re not fat. If they’re super skinny (skin and bone), we need them to understand that this is not realistic at all. Your expectations are not realistic.
Now, let’s take a look at the care plan for eating disorders, starting with the subjective data.
So, the patient with anorexia nervosa may have an obsession with calories or fat content on foods. They might look at that calorie content on the back of the box and just obsess over it like, oh, this is too many calories. This is because of their disturbed body image and their fear of gaining weight. So, those with bulimia nervosa might not be as obsessed with those calories, but instead they might disappear after they’ve eaten. This is because they’re going to vomit, right? So, This will prevent their body from absorbing the calories which they need, so the patient may also have a chronically sore throat. This is because of the repeated vomiting, so it might really be sore all the time. They might even have a scratchy voice. Patients with eating disorders, they are probably gonna show denial. They’re not gonna accept that they have a low body weight and they might be really fatigued and weak because they are not getting those nutrients that they need and they also might have a lack of muscle mass.
Now let’s talk about the objective data. The patient might notice that they’re restricting their eating. They’re just not eating very much at a time and they might not like to eat around people either. So, the patient may appear really emaciated, you know, really, really skinny, and they might have really brittle hair that breaks super easily, really thin and brittle. Their nails might break really easily. They might even have hair covering their body, which is called lanugo, which is so unusual, right? You think of that in babies, but this is because the body is attempting to protect itself. They’re so thin that they’re freezing, so they’re going to start getting hair to keep them warm. Then the patient might look really lethargic because remember, they’re not getting that nutrition that they really need for their body to function properly. The patient with binge eating disorder might eat really abnormally fast sometimes around you, but sometimes in secret, you might not even see it going on. Those with bulimia nervosa might eat normally fast as well, but then they disappear into another room so that they can purge.
Now, let’s talk about the nursing interventions for the patient with an eating disorder. You should assess the patient, taking notes on their skin, their muscle tone, neuro status and mental health. Obtain a baseline, know any deficits or issues that require prioritization,such as nutrition. That’s probably going to be your first priority. So you’ll want to get nutrition in them one way or another. You will assess the patient’s nutritional status and set a weight goal. This is so that you can determine if the patient is underweight or overweight and this is our little scale here, and remember to watch for food hoarding because sometimes they will, and also watch for disposal of food. These people can be really strategic in the ways that they handle their food. Make sure you supervise them during their meals and for one hour after in case they’re going to go purge. So, this is so that you can try to determine what their eating habits are and so you can prevent that purging, right? Provide small meals. Snacks are awesome because you know, throughout the day just do small meals, small snacks and even liquids because it’s a lot easier to digest and it’s easier for them to choose a simple liquid than try to figure out what they are going to eat? It’s going to make digestion easier. It’ll help to minimize the bloating.
You want to record weights and monitor their exercise program. This is so that you can monitor their progress and improve muscle strength and tone as they increase their caloric intake. You’re going to provide medication and TPN as appropriate. So TPN would be for really severe malnourishment. Other medications might need to be given for mental disorders that they have along with therapy. Provide education for the patient and the family. This is important because the family might be very involved in this patient’s life, so give them information about the disease, about treatment and resources. This is to help reduce stress and help them make decisions because this can be a really scary time for them.
We love you guys. Now go out and be your best self today and as always, happy nursing!