Mrs. Black is a 31 year old female who is 2 weeks postpartum. This morning her husband found her difficult to rouse and confused, and called 911. The husband indicates she has been quite anxious since the birth of their first child. He reports she has had nausea and vomiting for two days, as well as watery diarrhea and generalized abdominal pain. She hasn’t been able to breastfeed baby because she’s been too anxious. Husband denies any sick contacts or recent travel.
Critical Thinking Check
Bloom's Taxonomy: Application
What other medical history would you want to attempt to gather from the husband?
VIEW ANSWER
Any complications with the pregnancy or delivery?
Characteristics of vomit/diarrhea? Any bleeding?
Medical conditions
Medications taken on a daily basis
Allergies
Critical Thinking Check
Bloom's Taxonomy: Application
What initial nursing assessments should be performed?
VIEW ANSWER
Neuro assessment – Level of consciousness, pupils, strength/movements
Abdominal assessment due to diarrhea and vomiting, assess for any masses, tenderness, or guarding with palpation
Full set of vital signs
Skin assessment – color, temperature, condition
Heat and lung sounds and respiratory/airway status
Upon further questioning, the husband reports Mrs. Black has a history of Hyperlipidemia, Graves Disease, and asthma and takes simvastatin and propylthiouracil daily, plus her rescue inhaler when she needs it. Upon assessment, Mrs. Black is somnolent and only minimally responsive to painful stimuli. She is unable to answer orientation questions and just keeps repeating her husband’s name. The nurse notes redness to her eyes and swelling around her eyelids. Heart rate is rapid and irregular. Lungs have diffuse crackles bilaterally. Vital signs are as follows:
HR145 bpm
BP120/76 mmHg
RR32 bpm
Temp101°F
SpO289% on 4L nasal cannula
Critical Thinking Check
Bloom's Taxonomy: Analysis
What should the nurse’s first action be?
VIEW ANSWER
Neuro assessment – Level of consciousness, pupils, strength/movements
Abdominal assessment due to diarrhea and vomiting, assess for any masses, tenderness, or guarding with palpation
Full set of vital signs
Skin assessment – color, temperature, condition
Heat and lung sounds and respiratory/airway status
Critical Thinking Check
Bloom's Taxonomy: Analysis
Based on the information you have, what diagnostic laboratory tests would you anticipate the provider ordering?
VIEW ANSWER
Full metabolic panel for electrolytes, renal function, etc.
Thyroid panel
Complete blood count to assess for infection or occult bleeding
Arterial Blood Gas to assess oxygenation / ventilation / gas exchange
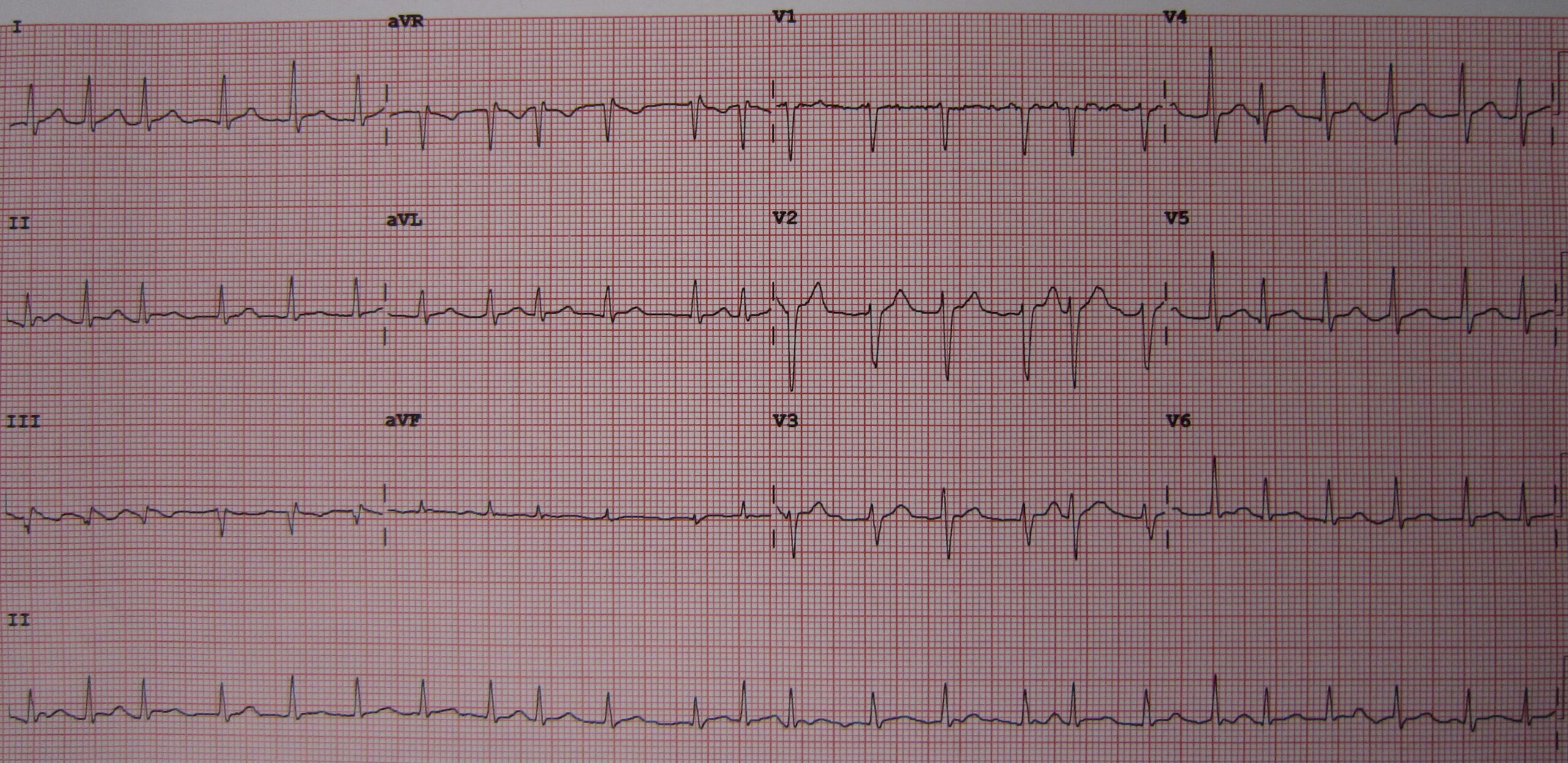
Mrs. Black becomes more obtunded and her heart rate goes up to 155. The provider orders a 12-lead EKG and proceeds to prepare for intubation for airway protection. The Respiratory Therapist comes to bedside and notes the patient has a swollen thyroid gland. For this reason, the Anesthesia team is called to the bedside to assist in a successful intubation. The provider orders a full lab panel, including CBC, CMP, LFTs, and a Thyroid Panel, plus an Arterial Blood Gas, and consults the ICU team to admit Mrs. Black.
This is the 12-lead EKG:
By James Heilman, MD – Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=19126125
Critical Thinking Check
Bloom's Taxonomy: Analysis
Interpret this EKG. What are the implications of this rhythm for the patient?
VIEW ANSWER
Atrial Fibrillation with Rapid Ventricular Response (rapid rate, >150)
This severe tachycardia with arrhythmia can be detrimental to the patient’s cardiac output, especially if this is not her baseline
It may also indicate underlying electrolyte abnormalities and/or other hormonal changes that are causing the severe tachycardia
No one’s heart can tolerate this fast blood pressure for that long
Critical Thinking Check
Bloom's Taxonomy: Analysis
What
VIEW ANSWER
Mrs. Black likely has a large goiter, this could cause obstruction of the airway and create for a difficult intubation.
The Anesthesia team is considered the expert consultants for airways within the hospital, most times. They are not only experts, but they can also bring equipment with them to assist with more difficult airways
Lab results return on Mrs. Black as she is transferred to the ICU:
Na144pH7.33TSH0.1
K5.0pCO248WBC 14K
Mg1.0HCO3–24Hgb12.5
BUN11pO2190 Hct38%
Cr0.7Lactate 3.2Plt450K
Critical Thinking Check
Bloom's Taxonomy: Analysis
What is going on physiologically with Mrs. Black?
VIEW ANSWER
Mrs. Black is likely experiencing a Thyroid Storm or Thyroid Crisis. This causes severe tachycardia and arrhythmias, N/V/D, and a severe febrile state.
Remember hyperthyroidism is ‘hypermetabolic’ – so now those things have become severe
The low TSH level is the clue that her thyroid hormone levels are likely sky high, you can count on that, even without the actual Thyroxine levels.
Critical Thinking Check
Bloom's Taxonomy: Analysis
What medications do you anticipate the provider ordering for Mrs. Black?
VIEW ANSWER
Beta blocker or calcium channel blocker to address the hypertension and tachycardia
Propylthiouracil or methimazole as antithyroid therapy
Any other medications required to address the symptoms during the crisis (antipyretics, antidiarrheals, antiemetics, etc.)
The provider orders a beta blocker and IV fluids for Mrs. Black, as well as an increased dose of propylthiouracil (PTU). She is stable for now, but it may take a few days for her to overcome this thyroid storm/crisis. Her husband asks the nurse what caused this.
Critical Thinking Check
Bloom's Taxonomy: Analysis
What is the best response to the husband to explain what triggered Mrs. Black’s Thyroid Storm/Crisis?
VIEW ANSWER
The stress of the pregnancy and delivery are likely the initial trigger.
The start of the Thyroid Crisis will have caused some anxiety for her and then continued to be further exacerbated due to excess stress